



Contact vous invite pour un moment convivial à la bastille avec un pique-nique sorti du sac.
RV au départ du téléphér...

38
Isère
Actualités & Agenda

20/06
La Marche des Fiertés de Grenoble édition 2026 se tiendra le samedi 20 juin au départ du Jardin de Ville.
Plus d'info...
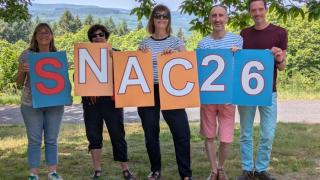
25/05
L'équipe de Contact Isère était présente le WE de Pentecôte au Séminaire National des Associations Contact (SNAC).
Le prog...
Juin 2026


LUNMARMERJEUVENSAMDIM
1 | 2 | 3 | 4 | 5 Permanence d'accueil et... 18h30 - 19h30 Centre LGBTI de Grenoble, 8 Rue Sergent Bobillot, 38000 Grenoble  | 6 | 7 |
| 8 | 9 | 10 | 11 | 12 Permanence d'accueil et... 18h30 - 19h30 Centre LGBTI de Grenoble, 8 Rue Sergent Bobillot, 38000 Grenoble | 13 | 14 |
15 | 16 | 17 | 18 | 19 Permanence d'accueil et... 18h30 - 19h30 Centre LGBTI de Grenoble, 8 Rue Sergent Bobillot, 38000 Grenoble | 20 | 21 |
22 | 23 | 24 | 25 | 26 Permanence d'accueil et... 18h30 - 19h30 Centre LGBTI de Grenoble, 8 Rue Sergent Bobillot, 38000 Grenoble | 27 | 28 |
29 | 30 | |||||
 Faire un don
Faire un don Adhérer
Adhérer Devenir bénévole
Devenir bénévole Intervention en milieu scolaire
Intervention en milieu scolaire Groupe d'écoute et de parole
Groupe d'écoute et de parole Accueil individualisé
Accueil individualisé Conviviale
Conviviale Brochures
Brochures visioconférences
visioconférences